Are people with asthma safer from COVID-19?


Among the many unknowns with COVID-19 is the severity of infection for people living with chronic respiratory conditions like asthma.
Conventional wisdom throughout the pandemic has been that anyone with a chronic condition is also likely to have an already-stressed immune system, which would lead to a greater risk of catching COVID-19 and of becoming seriously ill. However, a new study from Israel appears to show that people with asthma have lower susceptibility to the SARS-CoV-2 virus.1
This could be of critical importance as healthcare providers and policymakers grapple with decisions regarding vaccine distribution (and researchers continue to evaluate the efficacy of those vaccines).
People with asthma may be less susceptible to COVID-19 #
The headline data from the study are fairly impressive: A retrospective analysis of over 37,000 enrollees in an Israeli HMO who were tested for COVID-19 using PCR testing (considered the best available testing technique) found that 6.75% of those who tested positive for the virus also carried a diagnosis of asthma. This compared rather well with the 9.62% of those people who tested negative who also had been previously diagnosed with asthma.
With a p-value of less than .001, the study is considered statistically significant and the researchers assert that people with pre-existing asthma appear to be less susceptible to COVID-19 than the general population.
Interestingly, the group also found that people who smoked (or had a smoking history) also appeared to be less susceptible to the virus. Obviously, this kind of revelation has the potential to turn conventional wisdom on its head, so the authors made every effort to control for confounders, including medication history (antileukotrienes, inhaled corticosteroids, and long-acting bronchodilators), concurrent conditions, and demographic factors. Regardless of adjustment, the lower apparent risk persisted.
Why people with asthma may be less susceptible to COVID-19 #
The authors presented several potential reasons for their surprising findings. Their core hypothesis focused on angiotensin-converting enzyme 2 (ACE2). ACE2 is a protein that sits on the surfaces of a variety of cells found throughout the body and helps regulate blood pressure. It also acts as the gateway for the SARS-CoV-2 virus, serving as an attachment point for the pathogen as it works its way into the cell itself. On top of that, this occupation of the receptor prevents its normal operation, which in turn is thought to promote the inflammation and other symptoms associated with the COVID-19 illness. 2
In cases of asthma and respiratory allergies, ACE2 expression tends to be limited; thus, the thinking goes that with fewer places for the virion to ‘stick,’ there’s a lower chance of infection.
Possible confounding factors #
At a microbiological level this hypothesis makes sense. However, as always, the correlation shouldn’t imply causation. To their credit, the authors are quick to highlight this in their conclusions, but the nuance is frequently lost in the translation between a scientific publication and general health reporting. Therefore, it’s important to take a look at some of the other confounding factors that could potentially explain the unexpected results.
The lifestyles of people living with respiratory diseases #
First and foremost, it’s entirely possible the cohort of COVID-19-positive patients had fewer people with asthma simply because those same people were taking more serious precautions. This was not presented in the paper itself, but in a follow-up interview, the paper’s second author, Dr. Eugene Merzon, highlighted this possibility.3
This theory has also been advanced to help explain why the COPD population has, in general, been under-represented in COVID-19 cohorts4. Again, this makes a great deal of sense; people who have lived with chronic respiratory issues are already well-versed at avoiding irritants and triggers, and in general, are predisposed to taking precautions more seriously. Again, with the prevailing view being that COVID-19 would be, in the words of more than one person living with COPD, a “death sentence” if contracted, the stakes are high and minimizing risk a high priority.
Limited exposure, masking, and hygiene measures all reduce the relative risk of letting the virus get anywhere near the ACE2 receptors.
Could inhaled corticosteroids help protect against COVID-19? #
Another hypothesis advanced by Dr. Merzon was the potentially protective effect of inhaled corticosteroids (ICS).
ICS therapy in the setting of COVID-19 has been wildly controversial, with ongoing research continually refining precisely in which populations it may play a role. Currently, the consensus stands with the use of ICS in severe cases, and this paper doesn’t really do anything to shift that view. However, in his follow-up, Dr. Merzon reiterated that some concurrent studies have demonstrated that at least some ICS molecules have been shown to potentially reduce viral replication, which in turn could reduce the severity of COVID-19.5
Again, it’s important to point out that most trials and meta-analyses have not demonstrated any protective benefit at the population level. However, it does remain possible that all of these factors in concert may reduce the risk.
Defining asthma without spirometry or other diagnostic testing #
However, there is another possibility that goes largely unmentioned in the study and the follow-up: Diagnostic uncertainty.
According to the Subjects section of the paper, people were considered to have asthma if they had at least one asthma-related ICD-9 code in their chart, as well as evidence of prescription of one or more asthma-related medications over the previous 12 months. There is no mention of any diagnostic testing, such as a bronchial challenge test or even simple spirometry. In addition, any patient with a diagnosis code related to COPD was specifically excluded, which the authors go on to mention prevented them fromevaluating the risk of COVID-19 in this population, even though many with COPD also have significant inflammation.
Accurate diagnosis’ of chronic respiratory diseases #
Unfortunately, this means that the evaluation is wholly reliant upon the accuracy of the medical record. Clearly, no one sets out to create an erroneous record, but both under- and over-diagnosis are rampant throughout the chronic respiratory world. Asthma is notoriously tricky to diagnose, particularly in the relatively mild cases that Dr. Merzon and his team report comprised the majority of their cohort.
Several analyses put the rate of overdiagnosis in asthma at approximately 30%, meaning 1 in 3 of the cases that had ostensible protection against the virus may not have had any such protection at all.6 The rate of under-diagnosis is thought to be at least as bad, with up to the best available research indicating that somewhere between 30-50% of cases go undiagnosed, with symptoms instead attributed to one of the many other non-pulmonary conditions that can cause shortness of breath.7 Again, this fundamentally flawed data could significantly skew the final data analysis and throw the conclusions into doubt.
The importance of objective testing for a proper diagnosis #
As with many other observations that have percolated out of the pandemic, it is now abundantly clear that healthcare systems around the globe need to place much greater importance on objective testing rather than simply relying upon reported symptoms.
Proper diagnosis of asthma is a thorny issue even in the best of times, with inconsistent diagnostic standards disseminated by national and international agencies and the heterogeneous nature of the condition itself. However, as this study makes mention of using standards recommended by the Global Initiative for Asthma (GINA) for assessing the severity of asthma cases, then using GINA diagnostic recommendations seems a reasonable place to start.
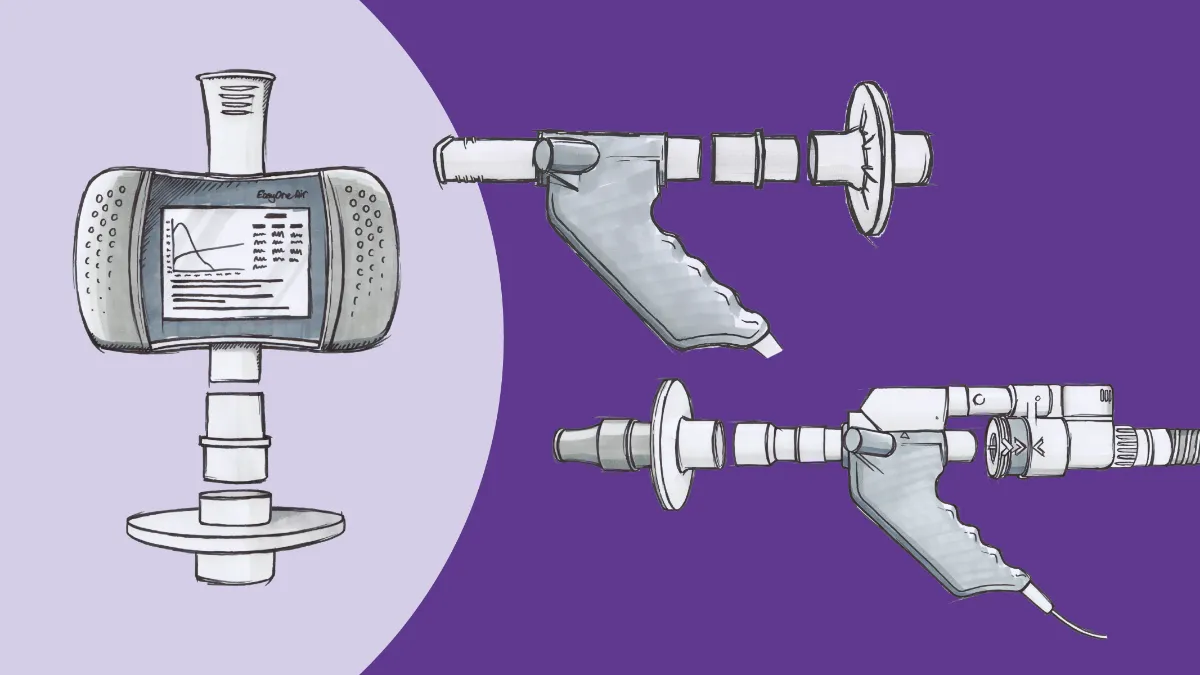
In their latest strategy report, GINA calls for a minimum of three steps for diagnosis: Reported symptoms typical of asthma, a detailed history that likely supports a diagnosis, and (critically) spirometry testing including evaluation of variable expiratory airflow obstruction.7 Most commonly (particularly in primary care), this would take the form of pre-and post-bronchodilator spirometry, where an improvement in the forced expiratory volume in 1 second (FEV1) of 12% and at least 200 mL would confirm variability (and strongly indicate asthma).
In light of that heterogeneity, though, GINA also provides several different alternatives, ranging from relatively involved (exercise challenges or bronchial challenges using inhaled irritants like cold air or methacholine) to basic and straightforward (serial peak expiratory flow measurements or repeated spirometry after a week of anti-inflammatory medication).
Greater access to spirometry can improve diagnosis accuracy #
Objective testing helps separate the wheat from the chaff and goes a long way to improving diagnostic accuracy.
Most of these tests are not terribly complex, either; with today’s technology, spirometry tests can be provided remotely, or in virtually any care setting, and inhaled bronchodilators are easy to come by. After some basic screening questions and pre-and post-bronchodilator spirometry, people with risk factors or symptoms consistent with asthma can be diagnosed within 20 minutes with a reasonable degree of confidence. Even better, many of these devices can be programmed with bronchial challenge protocols, making even advanced testing available in primary care offices, clinics, and other ambulatory settings.
This reduces the number of people who may otherwise get lost to follow up with pulmonology offices or busy pulmonary function laboratories, particularly important during times where such offices are already backed up with pandemic-related scheduling issues.
The far-reaching importance of easy, quick and accurate diagnosis #
Of course, the impact of bad input goes well beyond a single study. Failing to move past the use of assumption and supposition in diagnosis not only generates bad research data, it has a massive impact on patient care. Undiagnosed conditions, by definition, are untreated conditions, and erroneous diagnosis prevents any chance at early interventions that may limit disease progression. It also has the potential to generate wasteful spending by forcing clinicians to consider incorrect causes when it comes to disease management and places people at earlier risk of disability and death.
Similarly, while most respiratory medications are thought of as relatively benign, they do have very real potential side effects, and over-diagnosis exposes people to unnecessary risk (while again their treatments are aimed at the wrong targets). These concerns won’t go away at the end of the pandemic.
No clinician wants to be wrong, but at the same time, no clinician wants to unduly burden the people under their care. Add given time constraints, cost concerns, and the many non-clinical factors that can go into medical care, it becomes very tempting to allow ‘good enough’ to drive the diagnostic process.
Fortunately, there is an increasing number of resources that empower clinicians to not settle for good enough anymore. Advances in testing technology and refinements in diagnostic criteria have made objective testing much more accessible at every level, from both a logistical and economic perspective.
Accurate diagnosis is critical to accurate research #
In a healthcare world that is increasingly data-driven, it is becoming more and more important to ensure not only the integrity of the data but its accuracy. As research efforts mine reimbursement claims, medical records, and other retrospective data sources, it becomes critical for those datasets to be accurate.
If we cannot rely upon those data, we cannot rely upon the conclusions we draw from them, and there’s no longer any need to make do with ‘good enough.’
Green I, Merzon E, Vinker S, Golan-Cohen A, Magen E. COVID-19 Susceptibility in Bronchial Asthma. J Allergy Clin Immunol Pract. November 2020. doi:10.1016/j.jaip.2020.11.020 ↩︎
Sriram K, Insel PA. A hypothesis for pathobiology and treatment of COVID-19: The centrality of ACE1/ACE2 imbalance. Br J Pharmacol. 2020;177(21):4825-4844. doi:10.1111/bph.15082 ↩︎
People with asthma less likely to contract COVID-19: study | TheHill. https://thehill.com/policy/healthcare/528129-people-with-asthma-less-likely-to-contract-covid-19-study. Accessed December 4, 2020. ↩︎
Halpin DMG, Faner R, Sibila O, Badia JR, Agusti A. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir Med. 2020;8(5):436-438. doi:10.1016/S2213-2600(20)30167-3 ↩︎
Matsuyama S, Kawase M, Nao N, et al. The inhaled steroid ciclesonide blocks SARS-CoV-2 RNA replication by targeting the viral replication-transcription complex in cultured cells. J Virol. 2020. doi:10.1128/jvi.01648-20 ↩︎
Kavanagh J, Jackson DJ, Kent BD. Over-and under-diagnosis in asthma. Breathe. 2019;15(1):e20-e27. doi:10.1183/20734735.0362-2018 ↩︎
Karametos I, Tsiboli P, Togousidis I, Hatzoglou C, Giamouzis G, Gourgoulianis K. Chronic Obstructive Pulmonary Disease as a Main Factor of Premature Aging. Int J Environ Res Public Health. 2019;16(4):540. doi:10.3390/ijerph16040540 ↩︎